At the end of 2024, 39,992 CMPA members were family physicians (Type of Work 35, 73, 78 and 79).
The graph below compares the 10-year trends of medico-legal experiences between family physicians and all CMPA members. The cases include all civil legal actions or College complaints that the members were involved in and are not limited to pediatric cases.
What are the relative risks of a medico-legal case for family physicians?
- Family doctors, College (n=22,868)
- Family doctors, Legal (n=3,096)
- All CMPA, College (n=49,311)
- All CMPA, Legal (n=13,578)
Between 2015 and 2024, family physicians had significantly higher rates (p<0.0001) of College complaints1 when compared to all CMPA members.
In the same 10-year period, family physicians had lower rates (p<0.0001) of civil legal cases than all CMPA members.
What are your risk levels regarding medico-legal cases, compared to other family physicians?
Percentage of family physicians, 5-year case frequency
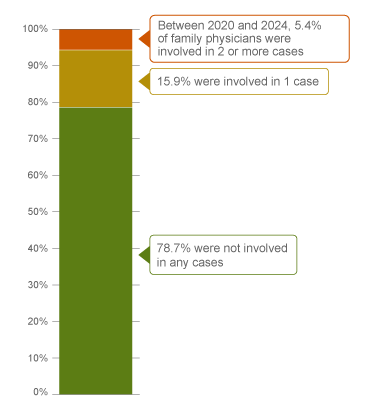
| No case |
78.7 |
| 1 case |
15.9 |
| 2 cases or more |
5.4 |
Percentage of family physicians, 1-year case frequency
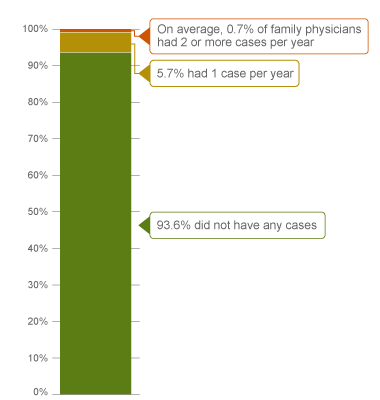
| No case |
93.6 |
| 1 case |
5.7 |
| 2 cases or more |
0.7 |
|
In a 5-year period (2020 - 2024)2, 16% of family physicians were named in 1 new medico-legal case, and another 5% were named in 2 or more cases.
Annually, 94% of family physicians did not have any medico-legal case. Of all family physicians, 0.7% had the highest frequency of 2 or more cases a year.
Pediatric care is one of the most frequent areas in medico-legal cases for family physicians. This resource focuses on family physicians caring for pediatric patients.
The following sections describe findings based on 916 cases closed by the CMPA between 2014 and 2024 involving family physicians providing pediatric care. For the purpose of this report, a pediatric patient is defined as a patient over 28 days of age and less than or equal to 18 years of age.
What are the most common patient complaints and peer expert3 criticisms? (n=916 cases)
| Deficient assessment |
39 |
19 |
| Diagnostic error |
32 |
21 |
| Unprofessional manner |
26 |
10 |
| Inadequate communication with patient or family |
18 |
13 |
| Failure to perform test or intervention |
15 |
9 |
| Inadequate office procedure |
14 |
11 |
| Failure to refer |
13 |
5 |
| Professional misconduct |
12 |
6 |
| Inadequate documentation |
9 |
26 |
| Inadequate consent process |
8 |
6 |
Complaints reflect the patient’s perception that a problem occurred during care. These complaints are not always supported by peer expert opinion. Peer experts may not be critical of the care provided or may have criticisms that are not part of the allegation by a patient, their family or guardian.
Inadequate communication between a physician and the patient, parents or caregivers is a frequent complaint and peer expert criticism. Examples of communication concerns include:
- The father of a preschool-aged child alleged that the family physician failed to obtain consent to provide care to his child. The parents were separated. The father had full legal custody. The mother had supervised visits and brought the child to see the family physician. The College was supportive of the family physician assessing the patient, noting that both parents had the right to seek medical attention for the child. The College also recommended that, in future, the family physician take the time to contact the father to get more information, which could have avoided the situation.
- Parents of a school-aged child with seasonal allergies alleged the physician failed to take the time to listen to the patient and parents’ concerns about their child’s symptoms, allowing only one complaint per visit.
- Parents of an adolescent patient alleged that the physician failed to inform the patient in a timely manner that she was leaving her practice and de-rostered the patient without providing adequate opportunity to find a new physician.
Inadequate documentation is a leading peer expert criticism. Examples include:
- Failure to document any support for the diagnosis of upper respiratory tract infection, any explanation of treatment choice of antibiotics, or any discussion about the relative benefits and risks of the intervention.
- Failure to document a physical assessment (including accessory muscle use and auscultation findings), to document whether an adult was present with the patient, or to document if they were being treated as a mature minor.
- Lack of detail in discharge plan related to asthma action plan, avoidance triggers, or review of previous investigations.
- Failure in obtaining informed consent regarding cryotherapy with liquid nitrogen, failure to document discussion regarding potential adverse side effects of the procedure, any difficulties that the patient may experience during the procedure, or follow-up care should the patient experience pain or blistering after the procedure.
What are the most frequent presenting conditions? (n=916 cases)
The table below shows the most frequent presenting conditions in 4 age group of patients: infants/toddlers not including neonatal patients (over 28 days old and under 2 years old), preschool-aged (2-4 years old), school-aged (5-12 years old), and adolescent (13-18 years old).
Infants/toddlers (28 days old to 2 years old, n=191 cases)
- Respiratory (e.g. acute upper respiratory, pneumonia)
- Ear (e.g. otitis media)
- Gastrointestinal (e.g. gastroenteritis)
Collapse section
- Musculoskeletal system (e.g. hip issues)
- Digestive system (e.g. pyloric stenosis)
Collapse section
- Head (e.g. contusions)
- Extremities (e.g. fractures)
Collapse section
Pre-school aged (2-4 years old, n=156 cases)
- Respiratory (e.g. upper respiratory)
- Ear (e.g. otitis media)
- Skin (e.g. molluscum contagiosum)
Collapse section
- Head (e.g. superficial lacerations)
Collapse section
School-aged (5 -12 years old, n=288 cases)
- Respiratory (e.g. upper respiratory)
- Ear (e.g. otitis media)
- Skin (e.g. viral warts, molluscum contagiosum)
Collapse section
- Behavioural and emotional (e.g. attention deficit and hyperactivity disorder)
- Anxiety/stress disorders (e.g. generalized anxiety, gender dysphoria)
Collapse section
- Head (e.g. wounds)
- Extremities (e.g. fractures)
Collapse section
Adolescents (13-18 years old, n=309 cases)
- Anxiety/stress disorders (e.g. generalized anxiety, gender dysphoria)
- Mood disorders (e.g. depression)
Collapse section
- Respiratory (e.g. upper respiratory)
- Skin (e.g. viral warts)
Collapse section
- Extremities (e.g. fractures)
- Head (e.g. concussions)
Collapse section
Frequencies of patients’ conditions among medico-legal cases are likely representative of physicians’ practice patterns and do not necessarily reflect high-risk conditions. There may be more than one patient condition documented on one case. One case may have more than one patient involved.
In 193 of the 916 cases, the patient experienced a diagnostic error, including misdiagnosis, missed or delayed diagnosis. In 119 of these cases, peer experts had a criticism of the physician’s deficient patient assessment. For example:
- A family physician failed to perform a comprehensive assessment to indicate that a cause for the patient’s pallor appearance could be anemia, resulting in the patient needing further investigations.
- A family physician failed to examine a female adolescent patient in person, or to perform an abdominal exam after the patient presented multiple times with persistent abdominal pain, contributing to the delay of a diagnosis of ovarian cancer.
Peer experts had a criticism of the physician’s inadequate knowledge or skill in 62 cases. For example:
- When a school-aged patient presented with a prolonged headache with eye pain, the family physician failed to seek urgent consultation or refer the patient to a pediatrician. Failure to request blood pressure or conduct a proper neurological exam contributed to a delayed diagnosis and treatment for cerebral venous sinus thrombosis with intracranial hemorrhage and cerebral edema.
- A family physician, treating a school-aged patient presenting with renal hematoma and recent abdominal trauma, failed to order the appropriate tests of imaging investigation (ultrasound or CT with contrast) and blood work (complete blood count). This contributed to a delayed diagnosis of a tumor.
What are the factors associated with patient harm4 in medico-legal cases? (n=916 cases)

Patient factors 5
Presenting with:
- Severe bacterial infections, including sepsis
- Meningitis and severe cranial infections
- Influenza and pneumonia
- Enlarged adenoids, allergic rhinitis
- Appendicitis
Infant/toddler presenting with:
- Symptoms of bradycardia, murmur
- Cough, dyspnea, wheezing symptoms
- Congenital malformations of the circulatory system
Adolescent presenting with:
- Diabetes mellitus
- Acute pharyngitis
- Endocarditis and cardiac arrest
- Mental and behavioural disorders due to psychoactive substance use
Provider factors 6
- Deficient assessment
- Failure to perform test/intervention (e.g. ultrasound or x-rays to further investigate for hip dysplasia)
- Failure to refer
- Choice of medication not optimal (e.g. under-prescribed dosage of dalteparin by 10x to treat a pulmonary embolism)
Team factors6
- Inadequate discharge instructions
Risk reduction reminders
The following risk management considerations have been identified for family physicians treating pediatric patients.
- Be mindful of certain illnesses and conditions presenting differently in pediatric patients. Engage in reflective practice to identify critical components of the physical examination for different patient age groups and developmental contexts, even when time is limited.
- Consider referring patients to a qualified specialist or the emergency department when you believe the required care is beyond your scope of practice or skill level. Notify patients, parents or caregivers in a transparent and timely manner if you decline to provide care while adhering to College guidelines. Explain the reason for declining.
- In cases of conflicting directions from parents, clarify the authority of each parent to consent on behalf of the child. Maintain a professional manner with both parents that is respectful and that recognizes the parents’ legal rights. When requesting copies of agreements or court orders regarding decision-making responsibility (custody) and parenting time (access), keep the copies on file.
- Provide comprehensive discharge instructions to patients, parents or caregivers, both verbally and in writing, including medications, follow-up care, symptoms/signs to monitor, and guidance on when to seek medical attention. Provide clear information on when and who to contact in case of complications. Confirm patients’, parents’ or caregivers’ understanding of the information being provided.
- Document in the medical record the patient's history (include symptoms and co-morbidities), physical exam findings, reassessments, differential diagnoses, investigations, diagnosis, and reasoning. Include any treatment plan and follow-up instructions you have shared with the patient, their parents or their caregivers.
Limitations
The numbers provided in this report are based on CMPA medico-legal data. CMPA medico-legal cases represent a small portion of patient safety incidents. Many factors influence a person’s decision to pursue a case or file a complaint, and these factors vary greatly by context. Thus, while medico-legal cases can be a rich source for important themes, they cannot be considered representative of patient safety incidents overall.
Now that you know your risk…
Mitigate your medico-legal risk with CMPA resources.
- CMPA Research:
- CMPA Learning:
Looking for more?
For any data request, please contact [email protected]
Notes
-
Physicians voluntarily report College matters to the CMPA. Therefore, these cases do not represent a complete picture of all such cases in Canada.
-
It takes an average of 2-3 years for a patient safety incident to progress into a medico-legal case. As a result, newly opened cases may reflect incidents that occurred in previous years.
-
Peer experts refer to physicians who interpret and provide their opinion on clinical, scientific, or technical issues surrounding the care provided. They are typically of similar training and experience as the physicians whose care they are reviewing.
-
In CMPA Research glossary, severe patient harm is defined as symptomatic, requiring life-saving intervention or major medical/surgical intervention, or resulting in a shortened life expectancy, or causing major permanent or temporary harm or loss of function.
-
Patient factors include any characteristics or medical conditions that apply to the patient at the time of the medical encounter, or any events that occur during the medical encounter.
-
Based on peer expert opinions. These include factors at the provider, team and system levels. For pediatric cases among family physicians, there is no evidence for any system level factors in the data.