At the end of 2024, 6,532 CMPA members were psychiatrists (Type of Work 36).
The graph below compares the 10-year trends of psychiatrists’ medico-legal experiences with those of all CMPA members.
What are the relative risks of a medico-legal case for psychiatrists?
- Psychiatry, College (n=4,018)
- Psychiatry, Legal (n=412)
- All CMPA, College (n=47,071)
- All CMPA, Legal (n=10,862)
Between 2015 and 2024, psychiatrists had lower rates of civil legal actions when compared to all CMPA members (P<.0001).
In the same 10-year period, psychiatrists consistently had significantly higher rates of College complaints1 than all CMPA members (P<.0001).
What are your medico-legal risk exposure, compared to other psychiatrists?
Percentage of psychiatrists, 5-year case frequency
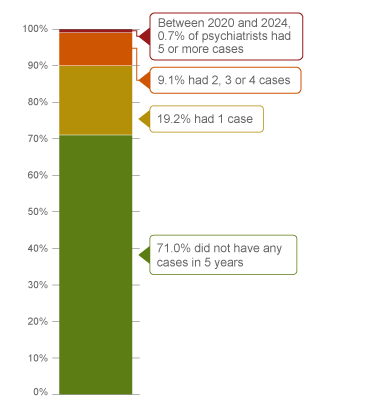
| No case |
71.0 |
| 1 case |
19.2 |
| 2, 3 or 4 cases |
9.1 |
| 5 cases or more (2020 - 2024) |
0.7 |
Percentage of psychiatrists, 1-year case frequency
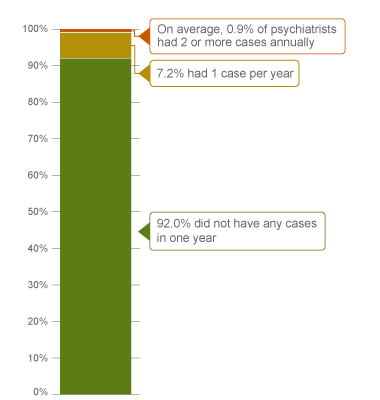
| No case |
92.0 |
| 1 case |
7.2 |
| 2 cases or more |
0.9 |
In a 5-year period (2020 – 2024)2, 90% of all psychiatrists were involved in either 1 or 0 medico-legal cases (including civil legal action, College and hospital complaints). Of all psychiatrists, 0.7% were involved in 5 or more new medico-legal cases in the 5 years.
Annually, less than 1% of all psychiatrists had 2 or more cases (the highest frequency of cases).
The following sections describe findings based on 1,324 civil legal actions, College and hospital complaints involving psychiatrists that were closed by the CMPA between 2020 and 2024.
What are the most common patient complaints and peer expert3 criticism? (n=1,324)
| Deficient assessment |
44 |
10 |
| Inadequate clinical decision making |
34 |
8 |
| Unprofessional manner |
28 |
10 |
| Professional misconduct |
24 |
4 |
| Diagnostic error |
24 |
5 |
| Inadequate documentation |
18 |
22 |
| Communication breakdown wih patient/family |
17 |
8 |
| Inadequate office procedure |
10 |
7 |
| Inadequte consent process |
9 |
4 |
| Inadequate monitoring or follow-up |
9 |
4 |
| Breach of confidentiality |
7 |
2 |
| Issues with professional boundary |
4 |
4 |
Complaints are a reflection of the patient’s perception that an issue occurred during care. These complaints are not always supported by peer expert opinion. Peer experts may not be critical of the care provided or may have criticisms that are not part of the patients’ allegation.
Patient allegations related to physicians’ professionalism were found in over 50% of the cases. These include unprofessional manner and professional misconduct. Peer experts had criticism on the psychiatrist’s professionalism in less than 20% of all cases. Examples of peer expert criticism of a psychiatrist’s unprofessional behaviours include:
- In treatment of depression, a psychiatrist initiated a new treatment medication of an antidepressant without first discussing the options of pharmacological treatment with the patient, who then experienced drug-induced psychosis, anxiety, and depression.
- A psychiatrist failed to address the patient's anxiety disorder with sufficient sensitivity. The peer expert criticized an inappropriate and condescending comment the psychiatrist made during the examination that the patient was “very sick.”
- A psychiatrist failed to establish a professional treatment relationship of mutual trust by critizing the patient’s behaviour, and made insensitive comments about the patient’s weight.
- A psychiatrist failed to maintain professional boundaries by sharing too much of their own personal information to a patient with post-traumatic stress disorder.
- A psychiatrist failed to read a psychoeducational assessment of a patient with an adjustment disorder, thereby not meeting the standard of practice in establishing a therapeutic doctor-patient relationship.
Inadequate documentation was the most frequent criticism by peer experts. For example:
- Documentation does not detail a complete mental status exam, or lacks the details that would support the diagnosis of the patient’s condition.
- Documentation that does not detail communication with the patient on matters such as their diagnosis, the reason for prescribing medications, potential side effects, and possible therapeutic impact.
What are the most frequent presenting conditions associated with psychiatric care? (n=1,324)
- Schizophrenia spectrum and other psychotic disorders (n=317)
- Depressive disorders (n=316)
- Anxiety disorders (n=224)
- Personality disorders (n=202)
- Bipolar and related disorders (n=172)
- Trauma- and stressor-related disorders (n=140)
Frequencies of presenting conditions among medico-legal cases are likely representative of psychiatrists’ practice patterns and do not necessarily reflect high-risk areas.
What are the factors associated with patient harm4 in medico-legal cases?

Patient factors5
- History of self-harm
- Presenting with or history of mental and behavioural disorders due to psychoactive substance use
- Recent visit to an emergency department
Provider factors 6
- Premature discharge of a patient from a health care facility
- Inadequate discharge planning (e.g. failure to ensure safety and follow-up plans were arranged and communicated to the patient and/or family members prior to discharge)
- Inadequate patient monitoring or follow-up
- Suboptimal choice of medication (e.g. failure to consider other medication interactions or potential side effects when prescribing medication)
Risk reduction reminders
The following risk management considerations have been identified for psychiatrists based on peer expert feedback:
- Facilitate shared decision-making with patient/substitute decision-maker (or family with consent) by providing clear information about diagnosis, treatment options, and expected outcomes; checking for understanding; and encouraging dialogue. Ask about patient’s goals, preferences and values before proposing treatment plans.
- In obtaining informed consent with pharmacotherapy or other treatment, discuss and document the diagnosis, proposed treatment, chances of success or anticipated results, treatment options (including non-treatment and its potential consequences), and material and special risks associated with the proposed and alternative treatments (including rare but important risks of major consequences). In the same discussion, ensure the patient's understanding and expectations, and answer any questions.
- Collaborate with the patient and, where appropriate, their support system in formulating a safety plan, particularly for any change or transition in care, including discharging a patient. Obtain collateral information if collecting the information directly from the patient is not reasonably possible.
- Ensure that clear and appropriate support and follow-up is arranged prior to discharge. Following discharge, review any red flags to watch for, and provide instructions on when to return for re-evaluation. Review and document a thorough mental status and risk assessment prior to transitions in care.
- Document in the medical record the patient's history (include symptoms and co-morbidities), mental health status, any suicidal ideation or homicidal ideation, physical exam findings, reassessments, differential diagnoses, investigations, diagnosis, and reasoning. Include any communication, treatment plan and follow-up instructions you have shared with the patient, their caregiver, or family.
Limitations
The numbers provided in this report are based on CMPA medico-legal data. CMPA medico-legal cases represent a small portion of patient safety incidents. Many factors influence a person’s decision to pursue a case or file a complaint, and these factors vary greatly by context. Thus, while medico-legal cases can be a rich source for important themes, they cannot be considered representative of patient safety incidents overall.
Now that you know your risk…
Mitigate your medico-legal risk with CMPA resources.
- CMPA Research:
- CMPA Learning:
Looking for more?
For any data request, please contact [email protected]
Notes
-
Physicians voluntarily report College matters to the CMPA. Therefore, these cases do not represent a complete picture of all such cases in Canada.
-
It takes an average of 2-3 years for a patient safety incident to progress into a medico-legal case. As a result, newly opened cases may reflect incidents that occurred in previous years.
-
Peer experts refer to physicians who interpret and provide their opinion on clinical, scientific, or technical issues surrounding the care provided. They are typically of similar training and experience as the physicians whose care they are reviewing.
-
Includes moderate, severe patient harm, and death. In the CMPA Research glossary, moderate harm is defined as symptomatic, requiring intervention or an increased length of stay, or causing permanent or temporary harm, or loss of function. Severe patient harm is defined as symptomatic, requiring life-saving intervention or major medical/surgical intervention, or resulting in a shortened life expectancy, or causing major permanent or temporary harm or loss of function.
-
Patient factors include any characteristics or medical conditions that apply to the patient at the time of the medical encounter, or any events that occur during the medical encounter.
-
Based on peer expert opinions. These include factors at the provider level. For cases involving psychiatrists, there is no evidence for team or system level factors in the data.