At the end of 2024, 151 CMPA members were thoracic surgeons (Type of Work 87).
The graph below compares the 10-year trends of thoracic surgeons’ medico-legal experience with those of all surgical specialties.
What are the relative risks of a medico-legal case for thoracic surgeons?
- Thoracic surgeons, College (n=77)
- Thoracic surgeons, Legal (n=35)
- All surgical specialists, College (n=7,497)
- All surgical specialists, Legal (n=3,569)
Due to the very small number of thoracic surgeons, their case volume fluctuated considerably year to year.
Between 2015 and 2024, the overall rates of College complaints1 and civil legal action for thoracic surgeons were significantly lower than the rate of all surgical specialties (p < .05).
What are your risk levels regarding medico-legal cases, compared to other thoracic surgeons?
Percentage of thoracic surgeons, 5-year case frequency
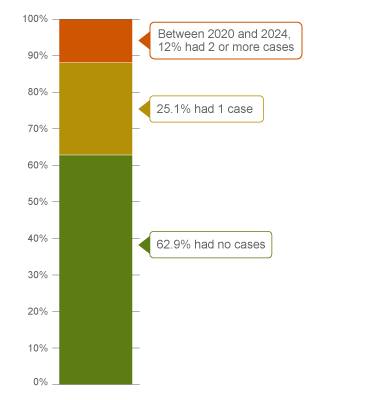
| No case |
62.9 |
| 1 case |
25.1 |
| 2 cases or more |
12.0 |
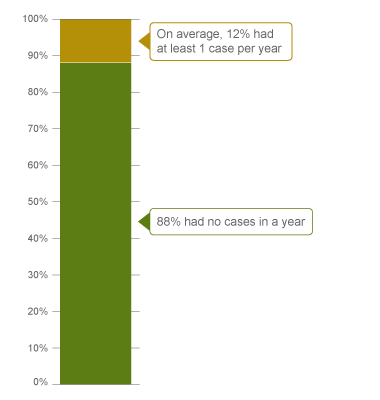
Percentage of thoracic surgeons, 1-year case frequency
In the past 5 years (2020 – 2024)2, 37% of thoracic surgeons were named in at least 1 new medico-legal case (legal action, College or hospital complaint).
Annually, 12% of thoracic surgeons were named in 1 or more new medico-legal cases.
The following sections describe the findings based on the 81 civil-legal cases, College, and hospital complaints involving thoracic surgeons that were closed by CMPA between 2015 and 2024.
What are the most common patient complaints and peer expert3 criticism? (n=81)
| Deficient assessment |
37 |
11 |
| Diagnostic error |
33 |
16 |
| Communication breakdown with patient/family |
25 |
12 |
| Inadequate monitoring or follow-up |
21 |
10 |
| Inadequate consent process |
18 |
4 |
| Failure to perform test or intervention |
18 |
10 |
| Injury associated with healthcare delivery |
14 |
6 |
| Poor decision-making regarding management |
9 |
3 |
| Failure to refer |
8 |
4 |
| Inadequate consent process |
8 |
8 |
Complaints are a reflection of the patient’s perception that an issue occurred during care. These complaints are not always supported by peer expert opinion. Peer experts may not be critical of the care provided or may have criticisms that are not part of the patients’ allegation.
Patient injury and diagnostic error were identified as both a patient allegation and as a peer expert criticism, where preventable harm was typically associated with multiple contributing factors such as loss of situational awareness and poor clinical decision-making.
Of the 81 patients, 14 incurred a healthcare-related injury. For example:
- A thoracic surgeon failed to review the complete CT report which documented a vascular anomaly. The surgeon proceeded with vessel ligation that was inappropriate for the patient’s anatomy. The patient experienced hypovolemic shock from the incorrect vessel ligation.
- A patient was injured at the trocar site when the laparoscopic instrument was removed following surgery, and developed respiratory distress, severe hypotension and anemia before leaving the OR. Peer experts criticized the thoracic surgeon’s delay in performing a laparotomy while waiting for laparoscopic equipment to investigate.
Diagnostic error was identified as an issue in 12 cases. For example:
- A patient's pancreatic cancer diagnosis was delayed when a thoracic surgeon failed to follow up on the CT scan results they had ordered while covering for another surgeon.
- A thoracic surgeon failed to diagnose an esophageal perforation in a patient after a hiatal hernia repair.
- A thoracic surgeon failed to follow up on the initial surgical pathology report indicating positive resection margins. As a result, the patient required additional, more extensive surgeries.
What are the most frequent interventions in medico-legal cases involving thoracic surgeons? (n=81)
| Intervention |
Patient count |
| Respiratory |
38 |
| Excision (e.g. lobectomy, wedge resection) |
23 |
| Biopsy |
8 |
| Bronchoscopy |
7 |
| Gastrointestinal |
21 |
| Excision (e.g. esophagectomy, gastrectomy) |
12 |
Intervention frequencies among medico-legal cases are likely representative of thoracic surgeons’ practice patterns and do not necessarily reflect high-risk interventions.
Frequent peer expert criticisms include:
Pre-operative phase
Inadequate consent process
- A patient experienced significant emotional distress after surgery as they were not aware that the surgery for hyperhidrosis may not provide permanent symptom relief.
- As part of the surgery consent discussion, a thoracic surgeon did not inform the patient that chronic thoracic pain is a common complication following an open thoracotomy. The patient later developed chronic pain post-operatively, which negatively impacted their quality of life.
Intra-operative phase
Misidentification of anatomy
- Misidentification of rib number resulted in large resection of the incorrect rib.
Failure to perform a test or intervention
- A patient developed a pulmonary embolism after a thoracic surgeon failed to resume anticoagulant therapy for DVT prophylaxis, despite the resolution of initial post-operative bleeding.
Post-operative phase
Inadequate monitoring or follow-up
- A thoracic surgeon failed to follow up on all pathology specimens, concluding the patient was cancer-free based solely on the initial report. A subsequent report revealed positive margins, resulting in a delayed diagnosis of recurrent cancer.
Inadequate documentation
- A thoracic surgeon failed to document follow up assessments and investigations, and to communicate to the patient’s other treating physicians that the patient’s post-operative symptoms were likely cardiac in nature and unrelated to the recent pulmonary surgery.
In addition, inadequate communication with the patient and/or family was the top criticism by peer experts and occurred in each phase of patient care. For example:
- The patient’s spouse arrived at the hospital only hours before the patient’s death, due to a lack of timely updates from the thoracic surgeon regarding the patient’s critical condition.
- A thoracic surgeon’s failure to address the patient’s questions and concerns led to a breakdown in communication and contributed to multiple complaints about mismanagement of care.
Risk reduction reminders
Gaps in non-technical knowledge or skills often lead to increased medico-legal risks and poor patient outcomes. The following risk management considerations have been identified for thoracic surgeons based on peer expert feedback:
Pre-operative
- Carefully consider the indications for the procedure, especially in high-risk patients. Consider arranging assistance for patients known to have challenging anatomy.
- In obtaining informed consent, discuss and document the following:
- the diagnosis
- the nature of the proposed treatment
- its chances of success
- alternative treatments (including non-treatment and its potential consequences)
- the material and special risks associated with the proposed and alternative treatments.
- Check for patient and, where appropriate, family or substitute decision-maker understanding. Ensure the discussion with the patient is clear, concise, and jargon-free, and provide sufficient time to address any patient questions. Document the discussion details in the medical record.
Intra-operative
- Anticipate the potential for intra-operative injuries by routinely having cognitive pauses, particularly during critical or complicated phases in a case. Injury to vital structures such as nerves and vasculature are prominent in medico-legal cases; document all efforts to visualize or protect these structures.
- Consider altering techniques or consulting a colleague when difficulties are encountered during surgery.
Post-operative
- Ensure there is a reliable system in place to facilitate the timely receipt, effective review and appropriate management and follow-up of investigative tests, including communicating results to patients. Evaluate and engage in quality improvement of the system for reliability and address quality gaps.
- Communicate details regarding ongoing monitoring to the patient and the responsible healthcare provider. Carefully document the patient’s condition, discharge instructions provided and details of the follow-up plan.
- Promptly disclose and inform patients of any complications or difficulties encountered during procedures or surgery. Discuss the implications, potential post-procedural or post-operative complications, and follow-up care with patients, ensuring open communication. Document these discussions in the medical record.
Limitations
The numbers provided in this report are based on CMPA medico-legal data. CMPA medico-legal cases represent a small portion of patient safety incidents. Many factors influence a person’s decision to pursue a case or file a complaint, and these factors vary greatly by context. Thus, while medico-legal cases can be a rich source for important themes, they cannot be considered representative of patient safety incidents overall.
Now that you know your risk…
Mitigate your medico-legal risk with CMPA Learning resources.
- CMPA Research:
- CMPA Learning:
Looking for more?
For any data request, please contact [email protected]
Notes
-
Physicians voluntarily report medico-legal matters to the CMPA. Therefore, these cases do not represent a complete picture of all such cases in Canada.
-
It takes an average of 2-3 years for a patient safety incident to progress into a medico-legal case. As a result, newly opened cases may reflect incidents that occurred in previous years.
-
Peer experts refer to physicians who interpret and provide their opinion on clinical, scientific, or technical issues surrounding the care provided. They are typically of similar training and experience as the physicians whose care they are reviewing.