At the end of 2024, 1,768 CMPA members were obstetricians (with or without gynecology, Type of Work 93).
The graph below compares the 10-year trends of obstetricians’ medico-legal experiences with those of all CMPA members.
What are the relative risks of a medico-legal case for obstetricians?
- Obstetricians, College (n=1,743)
- Obstetricians, Legal (n=977)
- All CMPA, College (n=49,331)
- All CMPA, Legal (n=13,582)
Between 2015 and 2024, obstetricians had significantly higher rates in both College complaints1 (p<0.0001) and civil legal actions (p<0.0001) when compared to all CMPA members.
What are your risk levels regarding medico-legal cases, compared to other obstetricians?
Percentage of obstetricians, 5-year case frequency
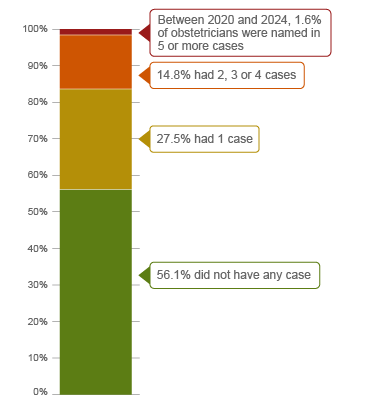
| No case |
56.1 |
| 1 case |
27.5 |
| 2-4 cases |
14.8 |
| 5 cases or more (between 2020-2024) |
1.6 |
Percentage of obstetricians, 1-year case frequency
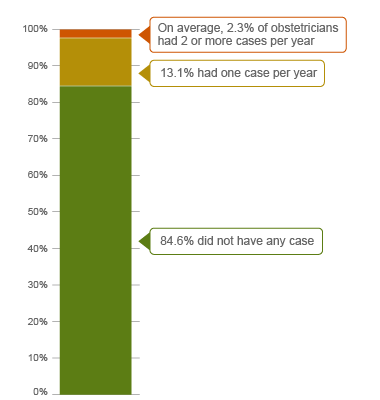
| No case |
84.6 |
| 1 case |
13.1 |
| 2 cases or more |
2.3 |
In a 5-year period (2020 – 2024)2, 44% of all obstetricians were named in at least 1 medico-legal case. 1.6% of obstetricians had 5 or more cases in this 5-year period (the highest frequency of cases).
On average, 15% of all obstetricians were named in at least 1 case per year between 2020 and 2024. 2.3% had an average of 2 or more cases per year.
In addition to obstetricians, physicians in other specialties, e.g. family physicians, also provide obstetric care to patients. The following sections present findings from 639 cases which include civil legal cases, College and hospital complaints, closed by the CMPA between 2020 and 2024, involving any physician who provided obstetric care.
What are the most common patient complaints and peer expert3 criticisms? (n=639)
| Deficient assessment |
45 |
22 |
| Failure to perform test/intervention |
45 |
22 |
| Diagnostic error |
36 |
30 |
| Inadequate communication with patient/family |
26 |
11 |
| Inadequate consent process |
25 |
9 |
| Unprofessional manner |
22 |
8 |
| Inadequate monitoring or follow-up |
18 |
9 |
| Poor decision-making regarding management |
17 |
8 |
| Inadequate monitoring or follow-up |
11 |
7 |
| Insufficient knowledge/skill |
16 |
16 |
| Failure to refer |
11 |
7 |
Complaints are a reflection of the patient’s perception that an issue occurred during care. These complaints are not always supported by peer expert opinion. Peer experts may not be critical of the care provided or may have criticisms that are not part of the patient allegation.
What are the most frequent interventions with peer expert criticism? (n=639)
- Cesarean section (n=161)
- Fetal heart monitoring during labour (n=115)
- Augmentation of labour (n=102)
- Operative vaginal delivery with forceps or vacuum (n=97)
- Induction of labour (n=71)
Intervention frequencies among medico-legal cases are likely representative of physicians’ practice patterns and do not necessarily reflect high-risk interventions. In addition to criticism related to the performance of these interventions, peer experts may criticize about a delay or an inappropriate use of these interventions (e.g. augmentation of labour with an abnormal fetal heart rate, forceps with a high head).
Fetal heart monitoring is an area often associated with diagnostic error. The most frequent peer expert criticisms related to fetal heart monitoring included:
- Delay or failure to perform an intervention.
- Peer experts were critical of the physician for failure to discontinue oxytocin augmentation despite the abnormal fetal heart tracing and uterine tachysystole, which led to uterine rupture.
- A physician’s failure to order continuous fetal heart monitoring when indicated for a high-risk patient, resulted in a delayed Caesarean section.
- Inadequate communication with other healthcare providers.
- An infant died when a resident failed to inform the obstetrician that the fetal heart rate was clearly abnormal with repetitive late decelerations and a low baseline.
- A nurse’s failure to clearly communicate concerns about the fetal heart rate led to a delayed delivery causing neurological injury to the infant.
- Misinterpretation of a test.
- An obstetrician misread the maternal heart rate for a normal fetal heart rate during labour, leading to delayed delivery and the birth of an infant with hypoxic-ischemic encephalopathy.
- Deficient clinical assessment.
- Peer experts were critical of the obstetrician for not assessing the patient sooner given patient’s prolonged labour, which led to hypoxic injury to the infant.
- Inadequate documentation.
- Peer experts were critical of the physician’s limited documentation and lack of a delivery note.
What are the factors associated with severe patient harm4 in medico-legal cases? (n=639)

Patient factors5
- ASA status 3+6
- Maternal age >35
- Multiple gestation
- Pre-eclampsia, eclampsia & HELLP syndrome
- Maternal infection (e.g. sepsis, obstetric wound infection)
- Abnormal bleeding and hemorrhage (e.g. placental abruption, immediate postpartum hemorrhage)
- Uterine rupture
Provider factors 7
- Deficient assessment
- Failure to admit (e.g. following atypical fetal heart rate finding)
- Failure to read medical records (e.g. biophysical profile, fetal heart rate tracings)
- Issues with intrapartum fetal monitoring
- Misinterpretation of fetal heart rate
- Failure to initiate internal fetal monitoring
- Deviation from clinical practice guidelines (e.g. SOGC guidelines for fetal health surveillance and induction of labour)
Team factors7
- Poor team communication related to an abnormal fetal heart rate
Risk reduction reminders
The following risk management considerations have been identified for physicians providing obstetric care based on peer expert feedback:
Antepartum
- Discuss each patient's individual labour and delivery options in the antepartum period and consider the possibility of unanticipated events requiring urgent or emergent interventions.
Intrapartum
- Clearly communicate persistent fetal heart rate concerns and clinical concerns to appropriate team members (e.g. OR team in preparation for a Caesarean section) and emphasize timely attendance of appropriate staff or delivery.
- Reinforce the need for regular training in fetal assessment and situational awareness for all obstetrics clinicians. Have clear policies for the interpretation and management of atypical or abnormal fetal heart rate tracings.
- Incorporate clinical pathways, clinical practice guidelines, or decision tools as appropriate.
Postpartum
- Be alert to potential postpartum complications when a patient repeatedly returns with the same or worsening symptoms. Reevaluate the diagnostic assumptions and repeat the physical examination. Consider whether to consult with a colleague.
- Following an obstetrical emergency, discuss the circumstances and outcomes with the patient and their family. Consult the CMPA handbook Disclosing harm from healthcare delivery, or contact CMPA for individual advice on disclosure.
- Debrief with the team following an urgent delivery or patient safety incident to evaluate the effectiveness of team communication. Document the care provided.
Limitations
The numbers provided in this report are based on CMPA medico-legal data. CMPA medico-legal cases represent a small portion of patient safety incidents. Many factors influence a person’s decision to pursue a case or file a complaint, and these factors vary greatly by context. Thus, while medico-legal cases can be a rich source for important themes, they cannot be considered representative of patient safety incidents overall.
Now that you know your risk…
Mitigate your medico-legal risk with CMPA Learning resources.
- CMPA Research:
- CMPA eLearning:
- CMPA Workshops:
Looking for more?
For any data request, please contact [email protected]
Notes
-
Physicians voluntarily report College matters to the CMPA. Therefore, these cases do not represent a complete picture of all such cases in Canada.
-
It takes an average of 2-3 years for a patient safety incident to progress into a medico-legal case. As a result, newly opened cases may reflect incidents that occurred in previous years.
-
Peer experts refer to physicians who interpret and provide their opinion on clinical, scientific, or technical issues surrounding the care provided. They are typically of similar training and experience as the physicians whose care they are reviewing.
-
Referring to both maternal and neonatal harm. In the CMPA Research glossary, severe patient harm is defined as symptomatic, requiring life-saving intervention or major medical/surgical intervention, or resulting in a shortened life expectancy, or causing major permanent or temporary harm or loss of function.
-
Patient factors include any characteristics or medical conditions that apply to the patient at the time of the medical encounter, or any events that occur during the medical encounter.
-
The American Society of Anesthesiologists (ASA) Physical Status Classification System is used by physicians to predict a patient’s risks ahead of surgery. ASA status 3 indicates severe systemic disease.
-
Based on peer expert opinions. These include factors at provider, team and system levels. For obstetric cases, there is no evidence for any system level factors in the data.